


 Sign Out
Sign Out

Hyaluronan is a polysaccharide found in the extracellular matrix of the subcutaneous tissue. It is depolymerized by the naturally occurring enzyme hyaluronidase. Unlike the stable structural components of the interstitial matrix, hyaluronan has a half-life of approximately 0.5 days. Hyaluronidase increases permeability of the subcutaneous tissue by depolymerizing hyaluronan. In the doses administered, hyaluronidase in DARZALEX SC acts locally. The effects of hyaluronidase are reversible and permeability of the subcutaneous tissue is restored within 24 to 48 hours.
Pharmacodynamics: NK cells express CD38 and are susceptible to daratumumab mediated cell lysis. Decreases in absolute counts and percentages of total NK cells (CD16+CD56+) and activated (CD16+CD56dim) NK cells in peripheral whole blood and bone marrow were observed with DARZALEX SC treatment.
Cardiac Electrophysiology: DARZALEX SC as a large protein has a low likelihood of direct ion channel interactions. There is no evidence from non-clinical or clinical data to suggest that DARZALEX SC has the potential to delay ventricular repolarization.
Exposure-Response Relationship: The exposure-response relationship and time course of pharmacodynamics of DARZALEX SC have not been fully characterized.
Clinical Studies: Newly Diagnosed Multiple Myeloma: In Combination with Bortezomib, Melphalan and Prednisone: The efficacy of DARZALEX SC with bortezomib, melphalan and prednisone was evaluated in a single-arm cohort of PLEIADES (NCT03412565), a multi-cohort, open-label trial. Eligible patients were required to have newly diagnosed multiple myeloma who are ineligible for transplant. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 6, once every 3 weeks from weeks 7 to 54 and once every 4 weeks starting with week 55 until disease progression or unacceptable toxicity; bortezomib 1.3 mg/m2 subcutaneously twice weekly on Weeks 1, 2, 4 and 5 for the first 6-week cycle (Cycle 1; 8 doses), followed by once weekly on Weeks 1, 2, 4 and 5 for eight more 6-week cycles (Cycles 2-9; 4 doses per cycle); and melphalan 9 mg/m2 and prednisone 60 mg/m2 orally on Days 1 to 4 of the nine 6-week cycles (Cycles 1-9). The major efficacy outcome measure was overall response rate (ORR).
A total of 67 patients received DARZALEX SC with VMP. The median age was 75 years (range: 66 to 86 years); 46% were male; 69% were White, 8% Asian, and 2% Black or African American; and 33% had ISS Stage I, 45% had ISS Stage II, and 22% had ISS Stage III disease.
Efficacy results are summarized in Table 1. The median duration of follow-up was 6.9 months. (See Table 1.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageRelapsed/Refractory Multiple Myeloma: In Combination with Lenalidomide and Dexamethasone: The efficacy of DARZALEX SC with lenalidomide and dexamethasone (DARZALEX SC-Rd) was evaluated in a single-arm cohort of PLEIADES (NCT03412565), a multi-cohort, open-label trial. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or unacceptable toxicity with lenalidomide 25 mg once daily orally on Days 1-21 of each 28-day cycle; and dexamethasone 40 mg per week (or a reduced dose of 20 mg per week for patients >75 years or BMI <18.5). The major efficacy outcome measure was ORR.
A total of 65 patients received DARZALEX SC with Rd. The median age was 69 years (range: 33 to 82 years); 69% were male; 69% were White, and 3% Black or African American; and 42% had ISS Stage I, 30% had ISS Stage II, and 28% had ISS Stage III disease. Patients had received a median of 1 prior line of therapy. A total of 52% of patients had a prior ASCT; 95% of patients received a prior PI; 59% received a prior immunomodulatory agent, including 22% who received prior lenalidomide; and 54% of patients received both a prior PI and immunomodulatory agent.
Efficacy results are summarized in Table 2. The median duration of follow-up for patients was 7.1 months. (See Table 2.)
 Click on icon to see table/diagram/image
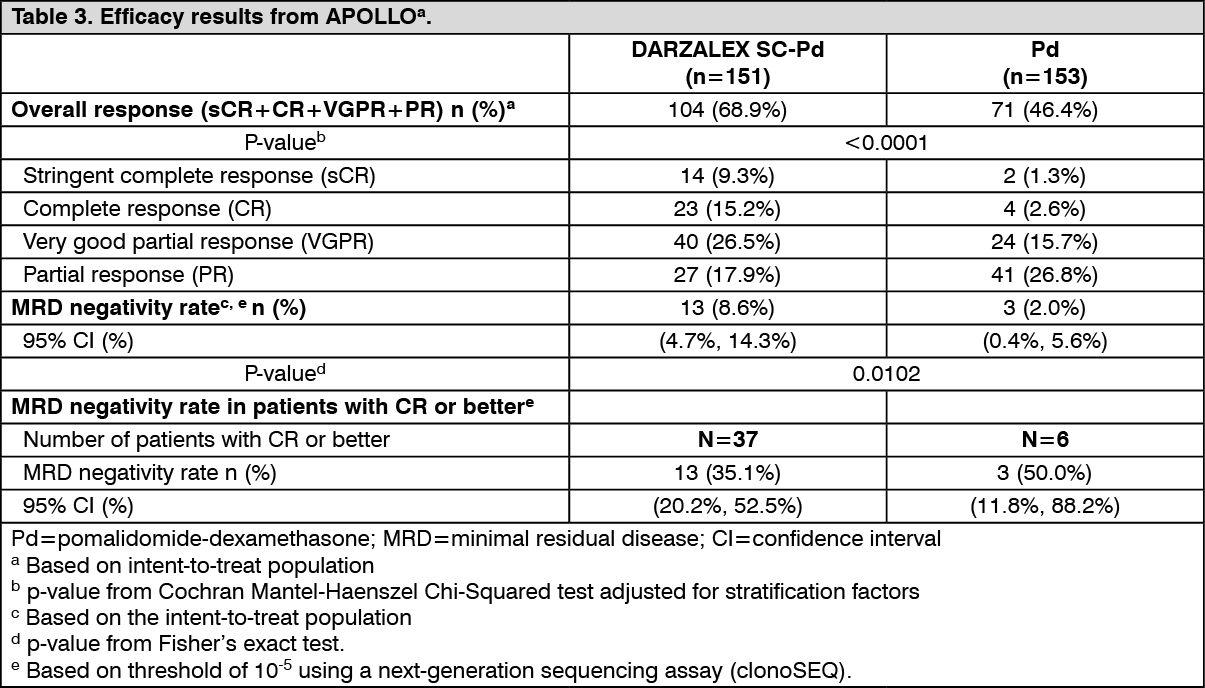
Click on icon to see table/diagram/imageIn Combination with Pomalidomide and Dexamethasone: The efficacy of DARZALEX SC with pomalidomide and dexamethasone (DARZALEX SC-Pd) versus pomalidomide and dexamethasone (Pd) alone was evaluated in APOLLO (NCT03180736), an open-label, randomized, active-controlled trial. Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or unacceptable toxicity with pomalidomide 4 mg once daily orally on Days 1-21 of each 28-day cycle; and dexamethasone 40 mg per week (or a reduced dose of 20 mg per week for patients >75 years). The major efficacy outcome measure was progression-free survival (PFS).
A total of 304 patients were randomized: 151 to the DARZALEX SC-Pd arm and 153 to the Pd arm. The median age was 67 years (range: 35 to 90); 53% were male and 89% were White, <1% were Black or African American, and <1% were Asian, and 45% had ISS Stage I, 33% had ISS Stage II, and 22% had ISS Stage III disease. Patients had received a median of 2 prior lines of therapy (range 1-5), with 11% of patients having received 1 prior line of therapy and 75% of patients having received 2-3 prior lines of therapy. All patients received a prior treatment with a PI and lenalidomide, and 56% of patients received prior ASCT. The majority of patients were refractory to lenalidomide (80%), a PI (48%), or both an immunomodulatory agent and a PI (42%).
APOLLO demonstrated an improvement in PFS in the DARZALEX SC-Pd treatment group as compared to the Pd treatment group; the median PFS was 12.4 months in the DARZALEX SC-Pd treatment group and 6.9 months in the Pd treatment group (HR [95% CI]: 0.63 [0.47, 0.85]; p-value = 0.0018), representing a 37% reduction in the risk of disease progression or death for patients treated with DARZALEX SC-Pd versus Pd. (See figure.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAdditional efficacy results from APOLLO are presented in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn responders, the median time to response was 1 month (range: 0.9 to 9.1 months) in the DARZALEX SC-Pd group and 1.9 months (range: 0.9 to 17.3 months) in the Pd group. The median duration of response had not been reached in the DARZALEX SC-Pd group (range: 1 to 34.9+ months) and was 15.9 months (range: 1+ to 24.8 months) in the Pd group.
With a median follow-up of 16.9 months, 99 deaths were observed; 48 in the DARZALEX SC-Pd group and 51 in the Pd group. Median OS was not reached for either treatment group.
In Combination with Carfilzomib and Dexamethasone: The efficacy of DARZALEX SC with carfilzomib and dexamethasone (DARZALEX SC-Kd) was evaluated in a single-arm cohort of PLEIADES (NCT03412565), a multi-cohort, open-label trial. This cohort enrolled patients with relapsed or refractory multiple myeloma excluding patients with left ventricular ejection fraction (LVEF) less than 40%, myocardial infarction within 6 months, uncontrolled cardiac arrhythmia, or uncontrolled hypertension (systolic blood pressure >159 mmHg or diastolic >99 mmHg despite optimal treatment). Patients received DARZALEX SC 1,800 mg/30,000 units administered subcutaneously once weekly from Weeks 1 to 8, once every 2 weeks from Weeks 9 to 24 and once every 4 weeks starting with Week 25 until disease progression or unacceptable toxicity with carfilzomib administered by IV infusion at a dose of 20 mg/m2 on Cycle 1 Day 1 and if a dose of 20 mg/m2 was tolerated, carfilzomib was administered at a dose of 70 mg/m2 as a 30-minute IV infusion, on Cycle 1 Day 8 and Day 15, and then Day 1, 8 and 15 of each cycle and dexamethasone 40 mg per week (or a reduced dose of 20 mg per week for patients ≥75 years or BMI <18.5). The major efficacy outcome measure was ORR.
A total of 66 patients received DARZALEX SC with Kd. The median age was 61 years (range: 42 to 84); 52% were male; 73% were White and 3% Black or African American; and 68% had ISS Stage I, 18% had ISS Stage II, and 14% had ISS Stage III disease. A total of 79% of patients had a prior ASCT; 91% of patients received a prior PI. All patients received 1 prior line of therapy with exposure to lenalidomide and 62% of patients were refractory to lenalidomide.
Efficacy results are summarized in Table 4. At a median follow-up of 9.2 months, the median duration of response had not been reached and an estimated 85.2% (95% CI: 72.5, 92.3) maintained response for at least 6 months and 82.5% (95% CI: 68.9, 90.6) maintained response for at least 9 months. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageMonotherapy: The efficacy of DARZALEX SC as monotherapy was evaluated in COLUMBA (NCT03277105), an open-label, randomized, non-inferiority study. Eligible patients were required to have relapsed or refractory multiple myeloma who had received at least 3 prior lines of therapy including a proteasome inhibitor and an immunomodulatory agent or who were double-refractory to a proteasome inhibitor and an immunomodulatory agent. Patients were randomized to receive DARZALEX SC 1,800 mg/30,000 units administered subcutaneously or daratumumab 16 mg/kg administered intravenously; each administered once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until unacceptable toxicity or disease progression. The major efficacy outcome measures were ORR by the IMWG response criteria and maximum Ctrough at pre-dose Cycle 3 Day 1 [see Pharmacokinetics as follows]. Randomization was stratified by body weight, myeloma type, and number of prior lines of therapy.
A total of 522 patients were randomized: 263 to the DARZALEX SC arm and 259 to the intravenous daratumumab arm. The median age was 67 years (range: 33 to 92 years); 55% were male; and 78% were White, 14% Asian, and 3% Black or African American. The median weight was 73 kg (range: 29 to 138). Patients had received a median of 4 prior lines of therapy. A total of 51% of patients had a prior ASCT; 100% of patients received both a PI and an immunomodulatory agent. Forty-nine percent of patients were refractory both a PI and an immunomodulatory agent. Eighty-two percent of patients were refractory to their last line of prior systemic therapy.
The results show that DARZALEX SC 1,800 mg/30,000 units administered subcutaneously is non-inferior to daratumumab 16 mg/kg administered intravenously in terms of ORR and maximum trough concentration [see Pharmacokinetics as follows]. Median progression-free survival was 5.6 months in the DARZALEX SC arm and 6.1 months in the intravenous daratumumab arm. ORR results are provided in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageLight Chain Amyloidosis: In Combination with Bortezomib, Cyclophosphamide and Dexamethasone: The efficacy of DARZALEX SC with VCd was evaluated in ANDROMEDA (NCT03201965), an open-label, randomized, active-controlled trial. Eligible patients were required to have newly diagnosed light chain (AL) amyloidosis with at least one affected organ, measurable hematologic disease, Cardiac Stage I-IIIA (based on European Modification of Mayo 2004 Cardiac Stage), and NYHA Class I-IIIA. Patients with NYHA Class IIIB and IV were excluded. Patients were randomized to receive bortezomib 1.3 mg/m2 administered subcutaneously, cyclophosphamide 300 mg/m2 (max dose 500 mg) administered orally or intravenously, and dexamethasone 40 mg (or a reduced dose of 20 mg for patients >70 years or body mass index <18.5 or who have hypervolemia, poorly controlled diabetes mellitus or prior intolerance to steroid therapy) administered orally or intravenously on Days 1, 8, 15, and 22 of each 28-day cycle with or without DARZALEX SC 1,800 mg/30,000 units subcutaneously once weekly from weeks 1 to 8, once every 2 weeks from weeks 9 to 24 and once every 4 weeks starting with week 25 until disease progression or a maximum of two years. When DARZALEX SC and dexamethasone were administered on the same day, dexamethasone 20 mg was administered before DARZALEX SC with the remaining dose of dexamethasone administered after DARZALEX SC if applicable. The major efficacy outcome measure was confirmed hematologic complete response (HemCR) rate based on Consensus Criteria as determined by the Independent Review Committee (negative serum and urine immunofixation, involved free light chain level decrease to less than the upper limit of normal, and normal free light chain ratio). Randomization was stratified by Cardiac Stage (European Modification of Mayo 2004 Cardiac Stage) countries that typically offer autologous stem cell transplant (ASCT) for patients with light chain (AL) amyloidosis, and renal function.
A total of 388 patients were randomized: 195 to DARZALEX SC-VCd and 193 to VCd. The median patient age was 64 years (range: 34 to 87 years); 58% were male; 76% White, 17% Asian, and 3% Black or African American; 23% had light chain (AL) amyloidosis Cardiac Stage I, 40% had Stage II, and 37% had Stage IIIA. The median number of organs involved was 2 (range: 1-6) and 66% of patients had 2 or more organs involved. Vital organ involvement was: cardiac 71%, renal 59% and hepatic 8%. The majority (79%) of patients had lambda free light chain disease.
Efficacy results are summarized in Table 6. (See Table 6.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe median time to HemCR was 59 days (range: 8 to 299 days) in the DARZALEX SC-VCd arm and 59 days (range: 16 to 340 days) in the VCd arm. The median time to VGPR or better was 17 days (range: 5 to 336 days) in the DARZALEX SC-VCd arm and 25 days (range: 8 to 171 days) in the VCd arm. The median duration of HemCR had not been reached in either arm.
The median follow-up for the study is 11.4 months. Overall survival (OS) data were not mature. A total of 56 deaths were observed [N=27 (13.8%) DARZALEX SC-VCd vs. N=29 (15%) VCd group].
Pharmacokinetics: Following the recommended dose of DARZALEX SC 1,800 mg/30,000 units subcutaneously once weekly for 8 weeks, the daratumumab peak concentration (Cmax) increased 4.8-fold and area under the curve (AUC0-7 days) increased 5.4-fold from the 1st dose to the 8th dose as monotherapy. Maximum trough concentrations for DARZALEX SC are typically observed at the end of the weekly dosing regimens for both monotherapy and combination therapies. The mean ± standard deviation (SD) maximum trough serum concentration (Ctrough) after the 8th dose was 593 ± 306 µg/mL when DARZALEX SC was administered as monotherapy and 537 ± 277 µg/mL, 526 ± 226 µg/mL, and 756 ± 276 µg/mL when DARZALEX SC was administered as combination with Pd, Rd, and Kd, respectively.
Table 7 lists the observed mean (±SD) maximum trough concentrations (Ctrough) after the 8th dose, simulated median (5th-95th percentiles) maximum Ctrough after the 8th dose, simulated median (5th-95th percentiles) Cmax after the 8th dose, and simulated median (5th-95th percentiles) area under the curve (AUC0-7day) after the 8th dose following DARZALEX SC 1,800 mg/30,000 units administered subcutaneously or daratumumab 16 mg/kg administered intravenously in patients with multiple myeloma or light chain (AL) amyloidosis. (See Table 7.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageAbsorption: At the recommended dose of DARZALEX SC 1,800 mg/30,000 units, the absolute bioavailability is 69%, with peak concentrations occurring around 3 days (Tmax) in patients with multiple myeloma. Peak concentrations occurred around 4 days in patients with light chain (AL) amyloidosis.
Distribution: The estimated mean (coefficient of variation, CV) volume of distribution for the central compartment is 5.2 L (37%) and peripheral compartment was 3.8 L in patients with multiple myeloma. The estimated mean volume of distribution was 10.8 L (28%) in patients with light chain (AL) amyloidosis.
Elimination: Daratumumab is cleared by parallel linear and nonlinear saturable target mediated clearances. The estimated mean (CV%) linear clearance of daratumumab is 119 mL/day (59%) in patients with multiple myeloma and is 210 mL/day (42%) in patients with light chain (AL) amyloidosis. The estimated mean (CV%) elimination half-life associated with linear clearance is 20 days (22%) in patients with multiple myeloma and 28 days (74%) in patients with light chain (AL) amyloidosis.
Specific Populations: The following population characteristics have no clinically meaningful effect on the pharmacokinetics of daratumumab in patients administered DARZALEX SC as monotherapy or as combination therapy: sex, age (33 to 92 years), renal impairment [Creatinine clearance (CLcr) 15 to 89 mL/min as determined by the Cockcroft-Gault formula], and mild hepatic impairment (total bilirubin 1 to 1.5 times ULN and AST>ULN). The effect of moderate and severe hepatic impairment on daratumumab pharmacokinetics is unknown.
Racial or Ethnic Groups: Of 190 patients with light chain (AL) amyloidosis who received DARZALEX SC and had a maximum Ctrough after the 8th dose, African-Americans (4%) had 24% higher daratumumab mean maximum Ctrough after the 8th dose compared to that of Whites (83%) and Asians (10%) had 16% higher mean maximum Ctrough after the 8th dose compared to that of Whites. The difference in exposure between that of Asians and Whites could be explained in part by differences in body size. The effect of African-American race on exposure and related safety and efficacy of daratumumab is unknown.
Body Weight: In patients with multiple myeloma who received DARZALEX SC 1,800 mg/30,000 units as monotherapy, the mean maximum Ctrough after the 8th dose was 12% lower in the higher body weight (BW) group (>85 kg), while the mean maximum Ctrough after the 8th dose was 81% higher in the lower BW group (≤50 kg) compared to the corresponding BW groups in the intravenous daratumumab arm.
In patients with light chain (AL) amyloidosis who received DARZALEX SC 1,800 mg/30,000 units in combination and had a maximum Ctrough after the 8th dose, the mean maximum Ctrough after the 8th dose was 22% lower in the higher BW group (>85 kg), while the mean maximum Ctrough was 37% higher in the lower BW group (≤50 kg) compared to the patients with body weight of 51-85 kg.
Toxicology: Preclinical Safety data: Carcinogenesis, Mutagenesis, Impairment of Fertility: No carcinogenicity or genotoxicity studies have been conducted with daratumumab. No animal studies have been performed to evaluate the potential effects of daratumumab on reproduction or development, or to determine potential effects on fertility in males or females.
No carcinogenicity, genotoxicity, or fertility studies were conducted for recombinant human hyaluronidase. There were no effects on reproductive tissues and function and no systemic exposure of hyaluronidase in monkeys given 22,000 U/kg/week subcutaneously (12 times higher than the human dose) for 39 weeks. As hyaluronidase is a recombinant form of the endogenous human hyaluronidase, no carcinogenicity, mutagenesis, or effects on fertility are expected.